


Seemingly out of nowhere, last week Republicans began seriously considering one last effort to destroy Obamacare. As with previous versions of Trumpcare, the legislation crafted by senators Lindsey Graham and Bill Cassidy faces two challenges: an absurdly short deadline — due to Senate procedure, they must act by September 30 — and resistance within the GOP to passing a bill that would impact one-sixth of the economy in unknown and likely devastating ways.
The senators are billing their legislation as a moderate approach, with Cassidy claiming, “A blue state can do a blue thing, a red state a red thing.” The reality is that it’s even more extreme that the GOP’s last few attempts to gut Obamacare. On top of all the draconian features of the previous bills, Graham-Cassidy shifts the burden of crafting a health care system onto the states, and makes them do it with far less money.
Here’s a look at what the legislation will do to the U.S. health-care system, if Senate Republicans can pick up another vote or two by next week.
Cut Protections for People With Preexisting Conditions
Under Graham-Cassidy, insurers could not refuse to cover someone because of a preexisting condition, but they would be able to make coverage so exorbitantly expensive that sick people couldn’t afford it.
First, insurance companies could charge people higher premiums based on their health status. The Center for American Progress estimates that annual premiums would be tens of thousands of dollars higher for a 40-year-old with various medical conditions than for a completely health person:
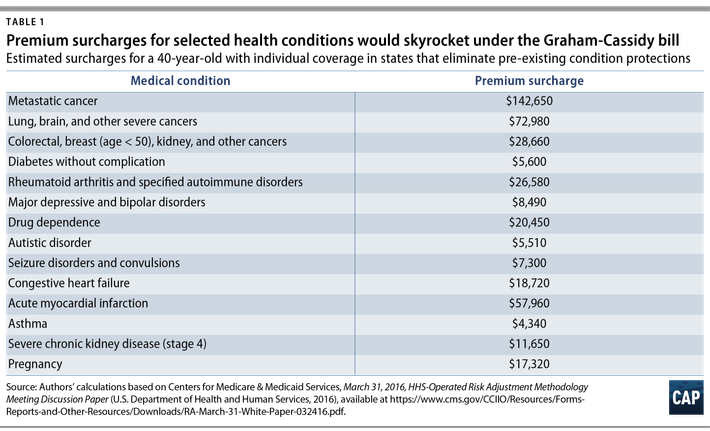
Obviously there are few of us who don’t have some sort of preexisting condition, and to make matters worse, under the bill someone who suddenly developed one of these conditions might find it’s not covered under their insurance plan. The bill also allows states to waive Obamacare’s essential health benefits, which require insurance plans to cover basics like hospitalizations, maternity care, and laboratory tests.
Conservatives like this because it would give people the freedom to buy skimpy health plans for dirt cheap, if that’s all they’re interested in. That would reduce costs for young and healthy people, but make comprehensive plans exorbitantly expensive since only sicker, older people would seek them out. (Like previous GOP health plans, insurers would be allowed to charge older people five times as much as younger people, while the currently limit is three times as much.)
States could theoretically opt to keep all of the current protections for people with preexisting conditions, and Republicans are pushing to have a vote before we get estimates of what each state would do. But as the Center on Budget and Policy Priorities notes, several months ago, the Congressional Budget Office scored a similar GOP proposal to let states waive these Obamacare provisions. The CBO concluded:
• States accounting for one-sixth of the nation’s population would choose to let insurers charge higher premiums based on health status. In those states, “less healthy individuals (including those with preexisting or newly acquired medical conditions) would be unable to purchase comprehensive coverage with premiums close to those under current law and might not be able to purchase coverage at all [emphasis added].”
• States accounting for half of the nation’s population would choose to let insurers exclude essential health benefits. In those states, “services or benefits likely to be excluded … include maternity care, mental health and substance abuse benefits, rehabilitative and habilitative services, and pediatric dental benefits.” People needing these services “would face increases in their out-of-pocket costs. Some people would have increases of thousands of dollars in a year.”
Gut Federal Funding for Health Care
Like any good Obamacare repeal plan, Graham-Cassidy would eliminate both the employer and the individual mandate. (Though states are free to reinstate them if they wish.) Multiple analysts have concluded that this would make health insurance more expensive, and lead to millions fewer being covered (some by choice, and some due to the aforementioned price increase).
But Graham-Cassidy does something even more radical: eliminating federal funding for Obamacare marketplace subsidies and the Medicaid expansion, and replacing it with one block grant to the states.
“If you like Obamacare, you can re-impose the mandates at the state level,” Cassidy told CNN. “You can repair Obamacare if you think it needs to be repaired. You can replace it if you think it needs to be replaced. It’ll be up to the governors. They’ve got a better handle on it than any bureaucrat in Washington.”
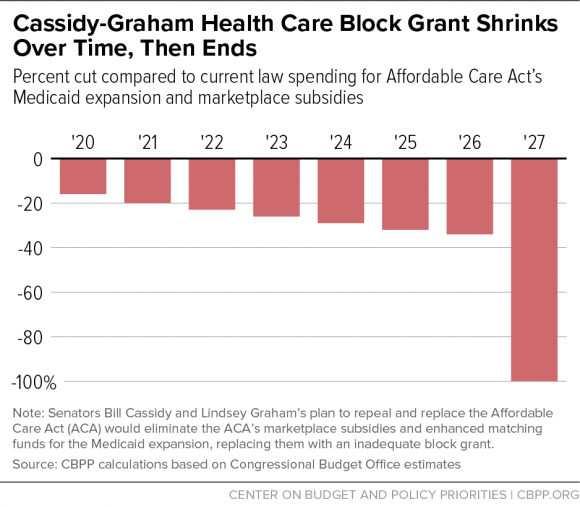
Indeed, states can basically put the money toward any health-care-related purpose. But Cassidy and Graham didn’t emphasize that the states will have far less money to create these new health programs. As the Center on Budget and Policy Priorities explains, between 2020 and 2026, states would receive less money via block grants than they would under Obamacare, and that gap would get worse over time:
The block grant would equal $140 billion in 2020, which is $26 billion, or 16 percent, below projected federal spending for the Medicaid expansion and marketplace subsidies under current law. The block grant would increase annually by roughly 2 percent, to $158 billion in 2026. That wouldn’t even keep pace with general inflation, which the Congressional Budget Office (CBO) projects to equal 2.4 percent annually over that period, let alone with expected growth in per-beneficiary health care costs and enrollment. Thus, by 2026, block grant funding under the plan would be $83 billion, or 34 percent, below currently projected federal spending on the ACA’s major coverage expansions.
This deficit wouldn’t hit states equally. The complex formula Graham-Cassidy uses to determine how much funding each state should get is designed not to “discriminate” against states that decided not to expand Medicaid. That means California, Connecticut, Delaware, Florida, Massachusetts, New Jersey, New York, North Carolina, and Virginia, and D.C. are likely to receive at least 50 percent less federal health funding by 2026.
“I think this is a game,” said Senator Rand Paul, one of the few GOP senators openly opposing the bill. “I think this is a game of Republicans taking money from Democratic states. What happens if Democrats take power back?”
If Graham-Cassidy were to remain in place, everything should even out in 2027, when the block grants disappear altogether. The bill’s sponsors claim the rules of budget reconciliation forced them to make the spending temporary, so in a decade millions would lose coverage if Congress fails to reauthorize the block grants.
Cut Medicaid Even Further
Graham-Cassidy would do even more to destroy Medicaid, fulfilling a longtime Republican dream. It includes a feature from the Senate’s previous version of Trumpcare: a per capita cap on federal funding for Medicaid. While the federal government currently pays a percentage of a state’s Medicaid costs, starting in 2020 it would pay a fixed amount for each Medicaid enrollee, regardless of what it actually costs to cover them.
States would have a number of other options — such as instituting work requirements and receiving part of their traditional Medicaid funding as a block grant — that would likely result in reducing eligibility and benefits for the poorest Americans. According to previous CBO estimates, non-expansion Medicaid funding would see a reduction of $39 billion, or 8 percent, by 2026.
Leave Millions Uninsured
The CBO score could prove fatal to Graham-Cassidy, as a handful of Republican senators killed previous efforts to repeal Obamacare over massive projected coverage losses.
The GOP’s plan to ram Graham-Cassidy through the Senate in the next two weeks could actually save it, since the CBO announced on Monday that it will not have time “to provide point estimates of the effects on the deficit, health insurance coverage, or premiums for at least several weeks.”
Presumably, Graham-Cassidy will be very difficult to score, since instead of creating a single Obamacare replacement, it could lead to a patchwork of 50 wildly different health-care systems. But we do know that the CBO previously estimated that a straight repeal of the Affordable Care Act would leave 32 million people uninsured and double premiums over the next decade. Compared to previous versions of Trumpcare, Graham-Cassidy gives states an even greater ability to cut preexisting-condition protections and tear apart Medicaid — plus it’s coupled with drastic cuts that set up a dramatic congressional showdown a decade from now. So, presumably, the new projections will be even worse.
On the plus side, it increases maximum contributions to health savings accounts, so there’s that.



























